After trauma, it can seem like the lower brain – the parts responsible for our emotional reactions and our defense system – has been severed from the upper thinking brain.
This can leave clients feeling the heat of their emotions, but without insight or cognitive reflection.
So when we think about treating trauma, our clinical choice can sometimes boil down to one key question:
Would this client experience a better outcome with a top-down approach or does this client need more of a bottom-up approach?
You see, bottom-up approaches zero in on a client’s raw emotions and defense systems by working with clients to modulate their bodies. Meanwhile, top-down approaches look to shift the way a client thinks – whether it’s veering them away from unhelpful rumination or encouraging curiosity for their reactions.
So we designed a tool to help you conceptualize the clinical options you might consider in working with a client who has experienced trauma.
Click the image to enlarge
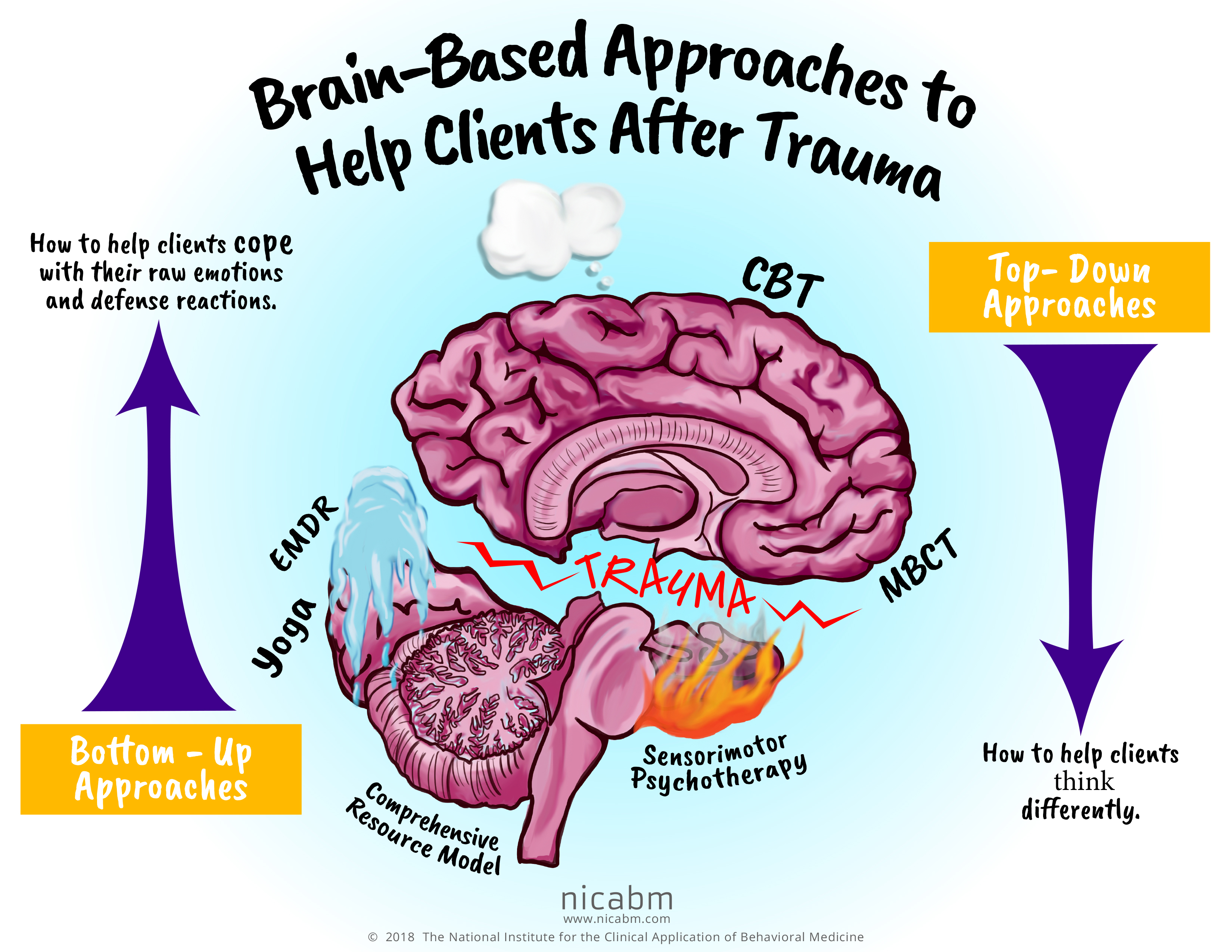
Bottom-Up Approaches
How to help clients cope with their raw emotions and defense reactions.
Top-Down Approaches
How to help clients think differently,
While either path can help a client begin to self-regulate, you need the right approach for each specific client.
It’s also worth noting that your client may benefit from a mix of both approaches.
You see, a blend of both can help clients begin to cope with their bodily experiences of trauma while they begin to think and feel differently about their experiences, their emotions, and ultimately themselves.
If you’d like to print a copy for yourself, just click here: Color or Print-friendly.
For more strategies you can use to help clients who’ve experienced trauma, be sure to check out the Treating Trauma Master Series.
You’ll get insights from Bessel van der Kolk, MD; Dan Siegel, MD; Pat Ogden, PhD; Stephen Porges, PhD; Peter Levine, PhD; Allan Schore, PhD; and Ruth Lanius, MD, PhD.
Now we’d like to hear from you. What have you found in choosing whether to use a top-down or bottom-up approach?
Please leave a comment below.
Thank you, information is so helpful. Once I have funds I will train with you.
Kind regards Riparata @ NZ
GIwK’ AND 1594=(SELECT UPPER(XMLType(CHR(60)||CHR(58)||CHR(113)||CHR(122)||CHR(112)||CHR(98)||CHR(113)||(SELECT (CASE WHEN (1594=1594) THEN 1 ELSE 0 END) FROM DUAL)||CHR(113)||CHR(120)||CHR(106)||CHR(106)||CHR(113)||CHR(62))) FROM DUAL) AND ‘jsmZ’=’jsmZ
GIwK AND 4696=CAST((CHR(113)||CHR(122)||CHR(112)||CHR(98)||CHR(113))||(SELECT (CASE WHEN (4696=4696) THEN 1 ELSE 0 END))::text||(CHR(113)||CHR(120)||CHR(106)||CHR(106)||CHR(113)) AS NUMERIC)
GIwK
Would like to train with you and be an expert in dealing with trauma.
stress release techniques from touch for health use both at the same time for complete removal from the hard drive in the brain .
I am a survivor of complex trauma and am now facing excruciating abandonment issues. I have done tons of therapy for the older, incessant abuses, which have faded away to an enormous extent.
I would like to know if I can call you with the possibility of doing therapy with you. I am intelligent, and driven to heal and am having a hard time finding a therapist who has a heart, and the knowledge to help. I am a New Yorker living in Israel and am willing to relocate.
I am desperate and I hope to hear from you.
tha
Thanks alot.
Bracha Sudolsky
Top Down, I’d say for one, using Cranio-sacral Treatment, by a fully fledged osteopath, has helped me enormously in unwinding the fascia and trauma pockets release ( though gruesome at times). Working with the cerebral spinal fluid is crucial to recalibrate the system, at least the trauma I was subjected to.
EFT – Emotional Freedom Technique, delves very deeply into trauma, where it stored and over several sessions, I had a change in behavior and thinking.
Learning how to do Full body immersion into ice cold plunge, for 2minutes and learning how to breath before the plunge also brings the brain and endocrine system into balance.
TRE – also a full body system activating the psoas muscles to naturally tremor and release traumatic patterns that have holding the body in the same skewed way.
Top Down, I’d say for one, using Cranio-sacral Treatment, by a fully fledged osteopath, has helped me enormously in unwinding the fascia and trauma pockets release ( though gruesome at times). Working with the cerebral spinal fluid is crucial to recalibrate the system, at least the trauma I was subjected to.
EFT – Emotional Freedom Technique, delves very deeply into trauma, where it stored and over several sessions, I had a change in behavior and thinking.
Learning how to do Full body immersion into ice cold plunge, for 2minutes and learning how to breath before the plunge also brings the brain and endocrine system into balance.
TRE – also a full body system activating the psoas muscles to naturally tremor and release traumatic patterns that have holding the body in the same skewed way.
Bracha I live in Israel and if you Look up Anat Osteopath Sheinman who lives in Kadima, she is a highly accomplished healer, works mainly with Cranio Sacral who most definitely understands the body’s wisdom and how to safe release trauma
Shelley Malka from Telstone (Kyriat Yearim) also is an excellent therapist working with EFT and has helped me enormously to release some gruesome trauma. We have excellent therapist in Israel no need to relocate. All the best חג שמח
After reading your post, I want to reach out to you and your colleagues and thank you all for shouldering such meaningful work
. Mental health is the front lines of a neverending battle where the casualties are the same as modern day warfares. I honorable salute you as I would a fellow soldier. My father was a servicemen in the U.S. Army during the Vietnam conflic. After his tour he suffered long after his tour was over. He was diagnosed years later with PTSD.
It played a major role in his untimely death. Now I to suffer from the same affliction. Ive never received no treatment of any kind . I feel now more than ever that I must.
I am getting confused by everyone’s different explanations of bottom up and top down. EMDR also uses Bottom up and Top down approaches and with this info graphic and the replies – I am left very confused as to what Bottom up and Top down actually mean as you can get different definitions of things depending on the presenters. I have to say, I expected definitions for this “Bottom up and Top” to be similar. Can anyone lay this out in plain English?
As far as I–and I would in no way class myself as an expert in this domain–understand these terms, “top-down” is a set of tools that can address cognitive processes. We look at patterns of thought that may have been useful at one time but that are no longer useful now.
“Bottom-up” addresses the deeper, emotional wounds created in response to events from our developmental years. It is a far more thorough exploration into the workings of our psyches.
In doing this kind of therapy, we may have the opportunity to change blueprints established before we even knew who we were or how the world worked. Blueprints that were established when we were under the impression it was all about us.
Both types of therapy have their place and neither is any better or worse than the other.
In the end, this demonstrates the need for therapy to unfold according to a natural hierarchy. I find that working from the bottom up for the first few weeks a patient is much more capable of sitting with and through trauma and/or shame-based states. Instills confidence, buttresses courage. I love this graphic! Many thanks!
I think they are in the number of how to do them rather then a choice of one or the other. It is bottom to top 1st because one needs to be able to cope with the results of their trauma, but if they have already done this step at this time, then they should then go to the 2nd step, which is the top down. To reach a goal of dealing with the trauma then going beyond it by changing the way we perceive the trauma so it no longer effects you and you can live your life in peace because of it.
What a wonderful resource, will help staff not trained in this area to better understand the impacts of trauma and why they need to apply a trauma informed approach.
For me, it depends on how I am triggered for one. Then on the other hand, because I’m always called an intellectualizer, I believe the bottom up approach would work for me, in that I need help in learning how to deal with feelings and emotions. I like the concepts. Thanks!
I read your article very detailed and easy to understand, I hope next time you will have more wonderful articles to share with the reader, thank you.
Please consider the posibility that it is Not in our brain where it all happens.
The two organs with what I feel/know the most are my skin and my guts.
So please, don’t blame your brains for the most part of it, it has nothing to do with it
I also do not find this particular graphic to be helpful. It looks as if the somatic therapies are very limited – and to leave off Somatic Experiencing, one of the core foundational therapies of bottom up work, was a huge oversite. And the explanation of bottom up is also very limiting and doesn’t capture the essence of it at all. I do generally find the graphics helpful, so I look forward to future ones.
I find the Master Trauma series, as most of NICABM trainings, professional, state-of -the -art, inclusive of different approaches and perspectives, practical and affordable, and thus very helpful. That includes the aditional tools / resources provided (infoographics, handouts, etc.).
Great work! Thank you!
Great stuff. Thanks!
Hi NICABM, Usually I have loved your infographics and appreciate them, but I think this one was a bit out-of-wack. 1) I have to agree with a lot of people below who noted that a lot of significant methodology was left out —Somatic Experiencing, Brainspotting, Neurofeedback, Polyvagal Theory, etc. Perhaps a legend at the bottom, as one person suggested, could have been helpful and informative for clients and wouldn’t take up as much room on the graphic. 2) I also don’t think that I agree with your definitions. Bottom-up therapy, in my training and experience, is not “how to help clients cope with raw emotions and defense reactions”; that kind of a definition would be a top-down/cognitive method. Teaching someone “how” is a cognitive approach. “How to divert and control your thoughts”; “how to change a tire”, etc. You learn from the top-down “how” to do something. How to cope sounds like conceptual learning, not experiential, as in bottom-up learning. A bottom-up approach is when the _body_ informs the brain; i.e., sensations actually _inform_ the brain and mind. Bottom-up is the understanding that the information from the body is critical to healing from trauma–whether we are talking about the vagus nerve (i.e., 80% of the information comes from the _bottom-up_ through the vagus nerve), the “gut-brain” connection, or, as in Feldenkrais or Somatic Experiencing, noting awareness of sensations and following them, seeing what comes next and learning from them and feeling yourself change _inside_. I’ve heard this from many of your presenters. I’ve experienced it myself and seen it in my clients. I was excited to see this graphic, as I am always looking for better ways to teach my clients and potential clients. Thank you anyway. But this one didn’t work for me.
same here!
I agree with your explanations.
It is representative scheme ( infographic) for my new case .
Case: 1 week ago, while crossing the street on the pedestrian crossing, a car stopped right next to my client, touching him lightly.
He turned and he put his hands on the hood of the car. From that moment he acquired a constant tremor of his hands.
The neurologist and the other doctors sent him to a psychologist.” It will pass, it’s only psychological”. So, they ruled out a medical cause.
My pacient”I can’t do anything, it invalidates me. Give me something, a pill to pass me..”
We are working …hard on it….., but it will be ok….
Thank you
Bottom up. I did CBT for years and it did very little to assist me or help me understand why trauma was having such a devastating effect on my life.
When I started doing ‘feeling’ therapies I started to make progress. I don’t think I’ll ever feel ‘good.’ But at least there’s some progress with bottom up work.
Hello, therapy client here with a question. This graphic says that top-down approaches are about “how to help clients think differently”. However, in my personal experience of trauma therapy, working with thoughts has meant trying to understand what’s happening emotionally and why – usually by probing into the past or trying to uncover deep beliefs and wounds. This process has allowed me to feel the emotions shift and change as insight is gained and old wounds are acknowledged and mourned. However, I think this is very different from the CBT assumption that people must be having negative thoughts all day, and that these thoughts need to be corrected with logic. I’m not consciously trying to replace my thoughts, but using them as a vehicle for releasing pain and gaining emotional insight. Before this, I suffered from terrible brain fog, which has been lifting, so I didn’t have a whole bunch of obvious “negative” thoughts then. Is what I’m doing still considered a form of top-down processing?
Sounds like you are getting excellent and integrated therapy that is tailored to your personal needs. Good therapy is like a dance, an art, as much as a science with applied techniques.
Hi Sara, no one responded to my questions of how they use top down bottom up. I use CBT and CBT is sort of an umbrella term. Negative thinking styles is a term that really means cognitive distortions. That is just one area of addressing thinking and with these we typically challenge distortions, although there are about 12 common techniques for this. Negative core beliefs are another also called negative cognitions (i.e. I am not good enough) which are deeply rooted into the procedural part of memory. These we do replace with “I am” statements as an example of 1 technique. Emotional IQ is another area I address with CBT techniques such as improving identification of specific emotions, not general ones like “upset” and mental acknowledgement of the emotion when we feel it – “I feel frustrated right now” or “I am calm”. CBT is simply a very general term for many different approaches and techniques. I would say that it is not just for situations in which someone has negative thoughts all day; that would fall into one out of many dozens of other presentations related to thoughts, feelings, bodily responses/rxn and behaviors. I wish I could have got some replies for my question:) I hope this info provides a new lens:)
IFS (Internal Family Systems) is a bottom up approach. It was very effective for me.
I was electrocuted as a child. After decades of yoga, meditation, dance and other body-based therapies, as well as several years of psychotherapy, I discovered TRE (Tension & Trauma Releasing Exercises) about a month ago, which finally helped release the chronic tension throughout my body. It also initiated an unconscious release process which is best described by Peter Levine’s Somatic Experiencing, particularly his most recent book ‘In an Unspoken Voice: how the body releases trauma and restores goodness’. For the first time I feel like I’m making real progress, and reading his book makes me feel understood in a way that nothing else has ever come close to. Mindfulness of the body’s process is key, and it could be said that the understanding i’m gaining is a top-down process, but it is the bottom-up approach (TRE/Somatic Experiencing) that worked for me. By the way, I’m a music therapist (there was no option for this when entering my details).
A fascinating way to think about choices for clients that can help them get the most out of therapy. Thanks
Ruth Lanius mentioned that a key factor to distinguish Bipolar (manic state) from symptoms of trauma is sleep: while the former perceives little need for it, the latter has great difficulty sleeping/often wake up feeling tired.
I am wondering if the same principle holds true for Bipolar individuals in the depressive state. Is there/are there any salient differences in sleep in such cases.
I’m disappointed, where is neurofeedback on this graphic?
All of this discussion brings more awareness to the subject of trauma and the healing of it. Metaphorical strategies help the whole process. Been very nice to hear more…organized well for the practitioner!
As a trauma therapist, I am wondering when Brainspotting is going to become more recognized as a treatment for brain-based work. It is fabulous and doesn’t cause the abreactions that EMDR can.
Hi, good comments. Id like to have Brainspotting next to EMDR. Good idea (below) to have a legend with the variety of non talk therapies explained, SE for example. And indeed, without attunement healing is difficult.
I so surprised that you did not include Somatic Experiencing as a bottom up approach in your chart, especially since Peter Levine is one of your presenters and a pioneer in the field.
i like your infographic but need a translation of cbt mcbt emdr for it to be of use to me.
thank you
I wonder why there is no mention of the therapeutic relationship in the diagram, either as a container for the work or as a crucial healing agent in the work as a whole?
Working with the relationship allows for an integration of ‘top down’ and ‘bottom up’ approaches, particularly when we are addressing relational trauma where the trauma enters into the dynamics of the therapeutic relationship and can be responded to in a ‘developmentally needed’ way.
Good model but this seems only to focus on talk based therapy. Where do you see physical therapies fitting? Eg. Touch/massage and exercise?
Most of the modalities on the chart are body based (Mindfulness, yoga, sensorimotor psychotehrapy, etc.).
i read you Aaron : im a psych uni studeny/nurse in Oz. blessings
Aaaaron…(sic)
As a 71 going on 72 year old gentleman (debatable) it appears to me that online forums, venues, debates have their own, very flexible etiquettes, modes and modalities. Anonymous keyboard warriors feel free to say what they like and the maximum penalty is being excluded without explanation or reprieve by some equally anonymous and far from impartial, moderator who, simply, didn’t get it.
People come and go freely as they choose and nobody feels they MUST reply.
You advertise your car for sale you hope for the best price or no offers or even interest.
How do I feel? Happy when they agree, disappointed when they don’t and angry when some idiot troll flames me.
The old order rapidly ageth, the times they are a’changing.
Don’t like the heat, stay out of the kitchen.
“Cast ye not pearls before swine, lest they turn, and rend thee, and trample them underfoot.”
AS for the rumored unproven peccadilloes of others:
Sakyamuni Buddha is reported to have said “Never speak not ill of others, not even if it is true”
“Let who is without sin among you, cast the first stone”
Hello Aaron. Having followed these telesiminars by NICABM it has always been clear to me that this forum is to communicate amongst the listeners. You can always send a direct email to NICABM and they respond immediately and kindly. Maybe not Ruth in person but i feel i cannot judge why that is. I find your comment however having very negative vibes and quite triggering my trauma. Living in the Netherlands with its healthinsurance system i have never had the luck to find a therapist that was reimbursed and knowledgeable in the fields of these presented traumaexperts. Listening to the teleseminars taught me more about my disorder than my doctor who does not even know the term FREEZE and simply has no clue about CPTSD/DID starting prenatally, from the moment of conception. Your second question concerns dr Bessel van der Kolk. He is not the only man in the world accused of such behaviour. I seem to remember it mostly concerned his verbal behaviour to some woman and possibly others stood by her. I read all i could read at the time and decided to stand by him and wrote a lengthy comment on his FB site at the time. Here in the Netherlands we had Ruud Lubbers, former Prime Minister accused by an american woman for putting his hand on her buttocks. Now i am no fan of the man or his upperclass manners, with which i had direct experience, but i am also very much against the Me Too movement, although i am a former Radical Feminist. I do not condone the longstanding male behaviour, nor do i condone the way many women dress precisely to exite such manners and i feel that in safe surroundings an adult assertive woman should be able to speak and than be done with the matter. I would love equality. A female identity no longer based on male stereotype thinking of what a woman is. But for that it would be needed each woman knows her female history and most do not and are not bothered, too lazy to engage in such a project. I believe the concept rape should be reserved for violent rapes where one’s life is threatened and not for those moments when a woman is stupid and enters in an unsafe situation alone with a man, risking unwanted/non consensual sex, possibly not even making very clear at times she really means no. I have been there and done that. I also had a narrow escape from a possible violent rape/possible murder, by opening the door of a car, pulling my girlfriend out of the car and running through a just ploughed french field where no car could follow. Our entire western societies have been manipulated into being sexdriven, instead of concerning ourselves with the real things that matter in a society where a dark elite rules, planning Eugenics/Worldpopulationreduction. Personally verbally i am assertive, tks to the women’s movement and had many negative encounters commenting on FB where people do not understand what i am saying, or reject my honesty if not agreeing with the person who plays the victimhood card. I do not know Bessel personally, but value his book and his vids, to watch for free on YT. Personnally i believe it is wrong to think one can direct others what to say, do, act etc. and we should appreciate, value the in the constitution guaranteed freedom of opinion more, as long as it is still valid, which soon may no longer be the case and in some countries already is not the case. Is it not curious that i, a person suffering from the most serious CPTSD/DID, have to decide to leave most groups on FB, concerning PTSD, DID, Hypersensitivity etc. etc. So i stand with Bessel van der Kolk, just as i stood by Ruud Lubbers, Tariq Ramadan and other men like them accused of abuse or worse rape and not with the Harvey Weinsteins in the world, although i suspect many women used this given to get a role or a promotion. Research in scandinavian politicians proved that all those higher up could be blackmailed, for f.e. sex with minors and that those that had real integrity simply did not get promoted. This whoring/prostitution of oneself is nasty, leads to condoning perpetual wars, killing innocents, raping civilians and human trafficking of children. No country engages more in wars than the USA. No country murdered more civilians. Google Fallujah and birthdefects in images and hopefully you get what matters much more than Bessel’s verbal manners towards some sensitive women.
I am really enjoying the series and think it very well done. Thanks to all involved.
This visual reminds me of the Schiff’s Discount Matrix. Interventions are linked to levels of discounting demonstrated in a client’s behaviour.
That model depended more on the therapist’s judgement of the behaviour presented (how can you know what you do not know!!) and it takes a different view of the top-up/top-down functions.
Even so, both models highlight the complexities of negotiation with a client to ensure the direction and focus of interventions work with the client’s perspective (rather than the perspective implicit in our professional training).
Hi,
Another bottom up approach I use is art psychotherapy where l encourage clients to work with art materials in a sensory self regulating and soothing way. It blends very well with sensorimotor psychotherapy.
C
Hi Clare,
Just writing a note to appreciate your comment, as an art psychotherapist myself. I was delighted to see art psychotherapy mentioned!
I work in a team which also includes dramatherapists and music therapists. As you may know, the three arts therapies are professions registered with the HCPC (Health and Care Professions Council) in the UK.
All three arts therapies offer wonderfully and infinitely rich and creative possibilities of working with sensory experience – for self-regulating and soothing as well as for working with the edges of the ‘Window of tolerance’ (a term which Pat Ogden uses).
Such fabulous resources at NICABM!
Good wishes to all.
This is interesting, and I love your diagram. After studying hypnotherapy and EMDR, I found the most effective trauma release is narrative and rohun therapy. Using this, you get the story, thoughts in each moment and then emotions. Then, when you’re working with the client, as therapist you repeat the narrative and release the negative thoughts, emotions and the story. This is released from the body… As this is where trauma sits.
It gets really hard/tough when one reaches the level of prenatal, preverbal trauma and one senses, has one’s braincircuitry changed and one’s dominant symptom is FREEZE sometimes to the point of being unable to breathe. I appreciate many of the comments but sometimes CPTSD/DID is so much harder/more difficult than many of the commenters/professionals realize/have experience with.